ROLE FIRST, FEATURE SECOND
A receptionist managing waiting rooms and a doctor triaging risk solve different problems. Designing for the role, not the feature, is what turns a database with a UI into software the team trusts.
W.01 — KARAZ CARE · HEALTHTECH · ENTERPRISE SAAS
Designed Karaz Care, a multi-role healthcare platform. Live in 13+ countries managing 100K+ patients. I led design end to end — research, information architecture, user flows, wireframes, the design system, and the final UI across five role-based dashboards — and managed two junior designers on the team.
THE THINKING
Diabetes care touches five different jobs in a clinic. Each role makes different decisions and needs different data. Before designing a single screen, I anchored the platform to four principles. Every fork in the road came back to these.
A receptionist managing waiting rooms and a doctor triaging risk solve different problems. Designing for the role, not the feature, is what turns a database with a UI into software the team trusts.
When clinicians see 100+ patients a day, the win is not more dashboards. It is a system that points at the few that need attention right now.
A risk badge without the why is just another thing to interpret. Every flag explains itself in plain language, with the data that triggered it.
A patient overview that lists every past lab is no longer an overview. Recent data, then a clear path to the full archive.
SCOPE OF WORK
Across the entire surface of the product — from research synthesis to design system.
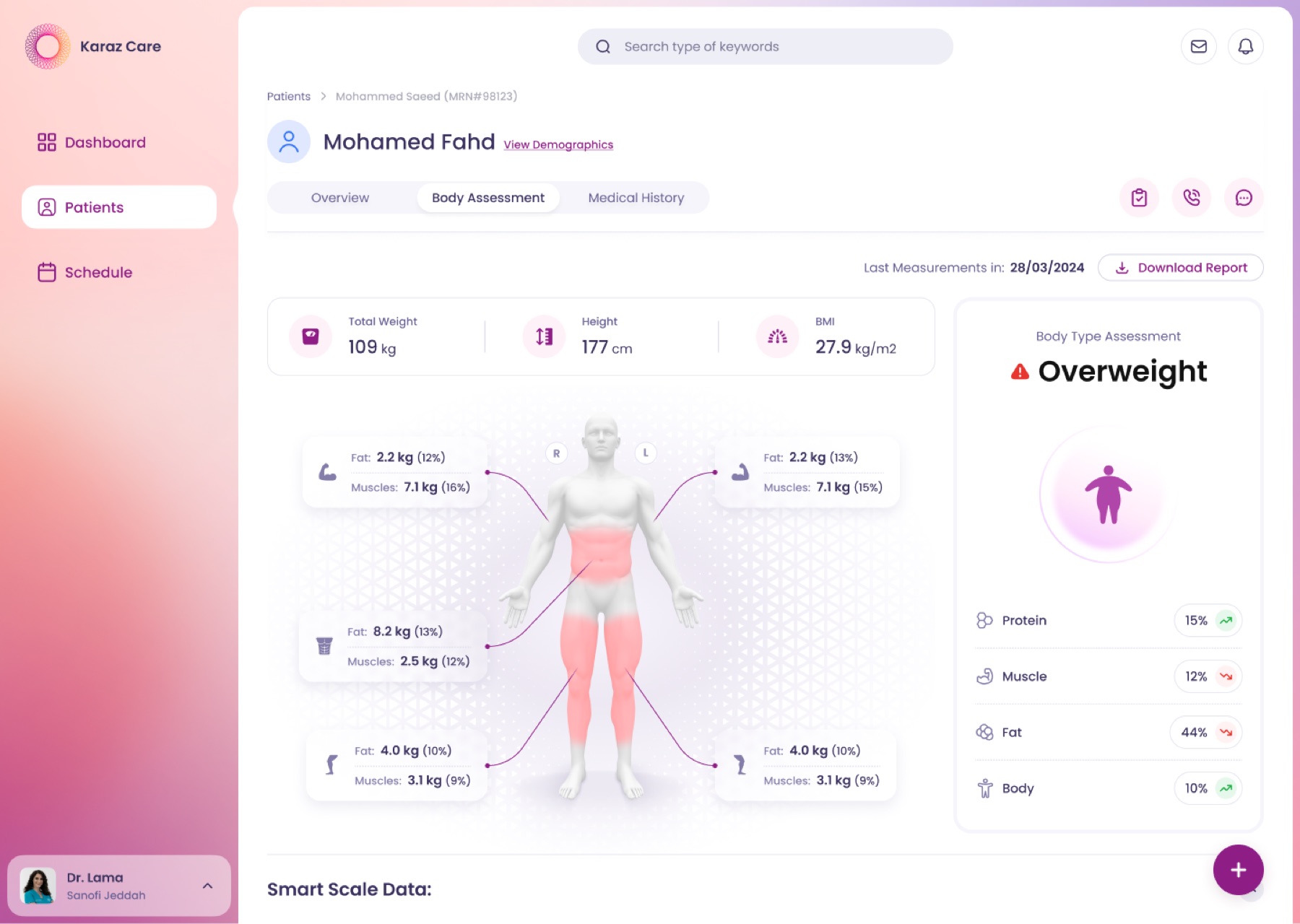
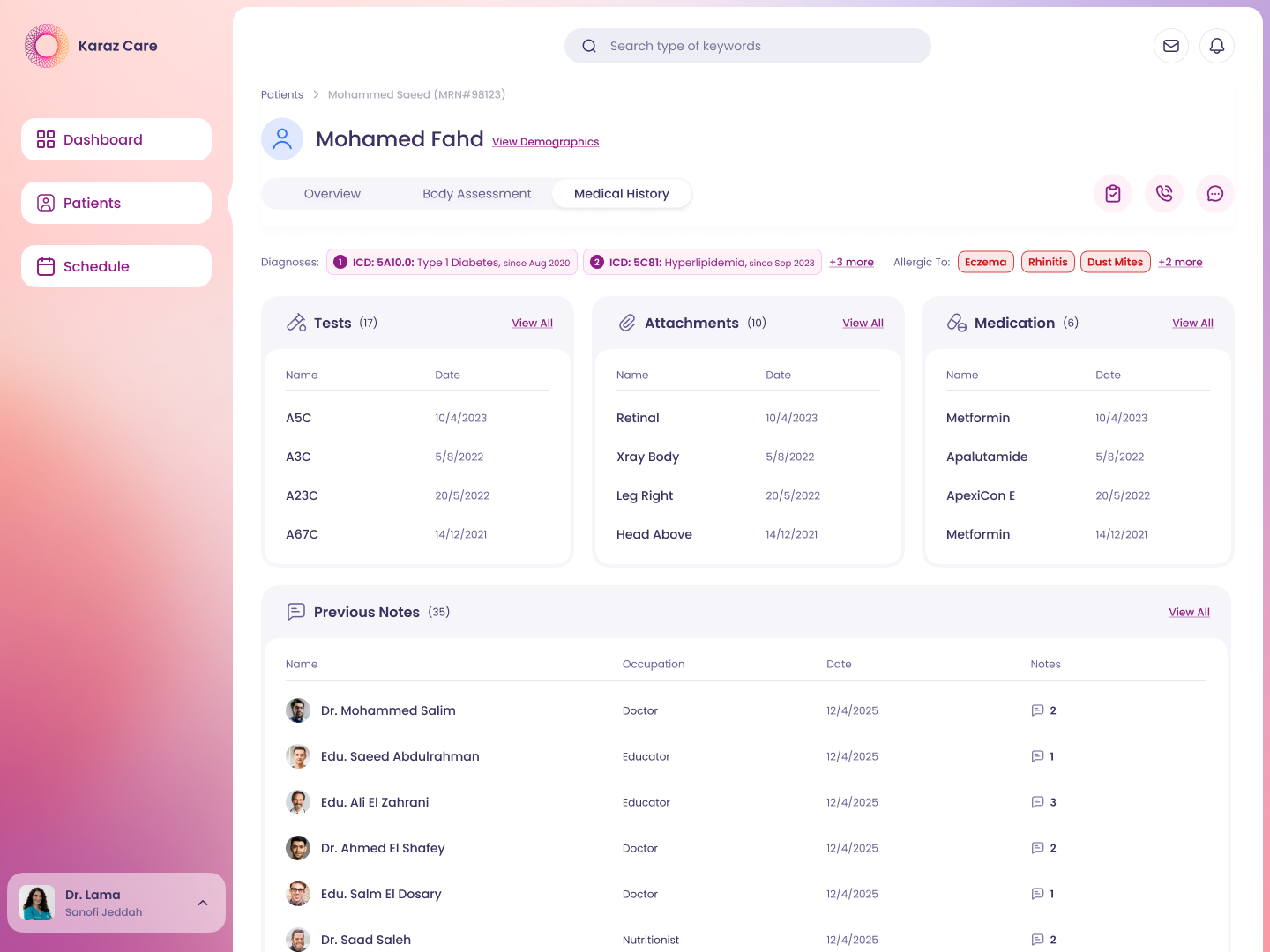
Risk triage, body assessment, glucose curves, AGP charts, full medical history.
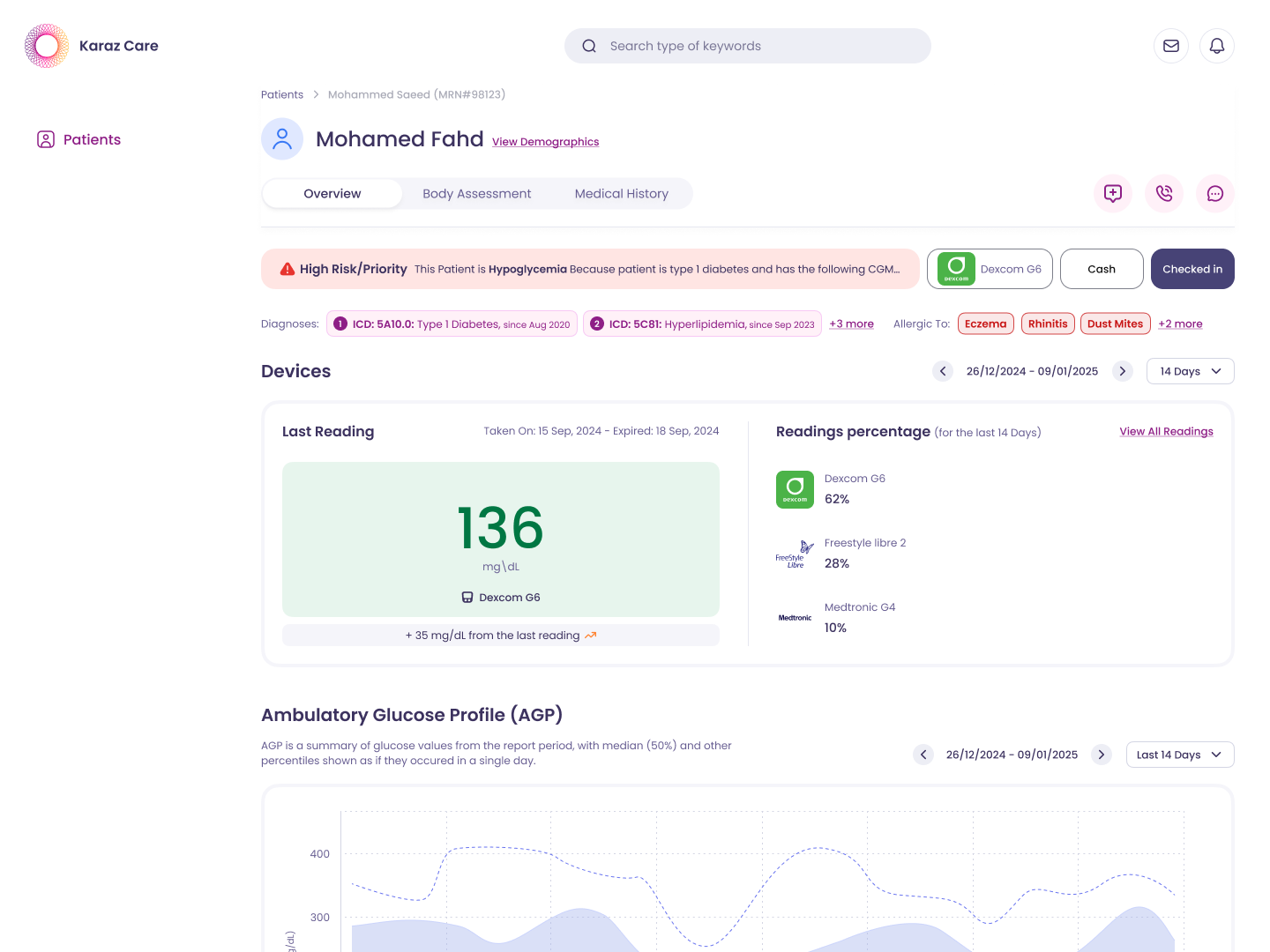
CGM device replacement workflow. Sensor lifecycle, replacement queue, courier handoff.
Role-based access. Doctors at one clinic don't see another clinic's data.
Clinician-patient and care-team messaging. Threaded by patient, archived for compliance.
Role-aware alerts and calendar. A doctor sees risk escalations, a receptionist sees check-in delays.
Colors, typography, components, and icons. One library, used by every screen across every role.
THE PROBLEM
Diabetes care was reactive and fragmented. Clinicians, nurses, receptionists, pharmacy staff, and admins all worked in separate tools. Patient data was stuck in handwritten logs and scattered reports. Karaz needed one connected platform where every role could see what mattered to them and act on it. A study of 384 patients over 3 months showed the real bottleneck. Not missing data. Too much raw data with no way to triage.
FIVE ROLES
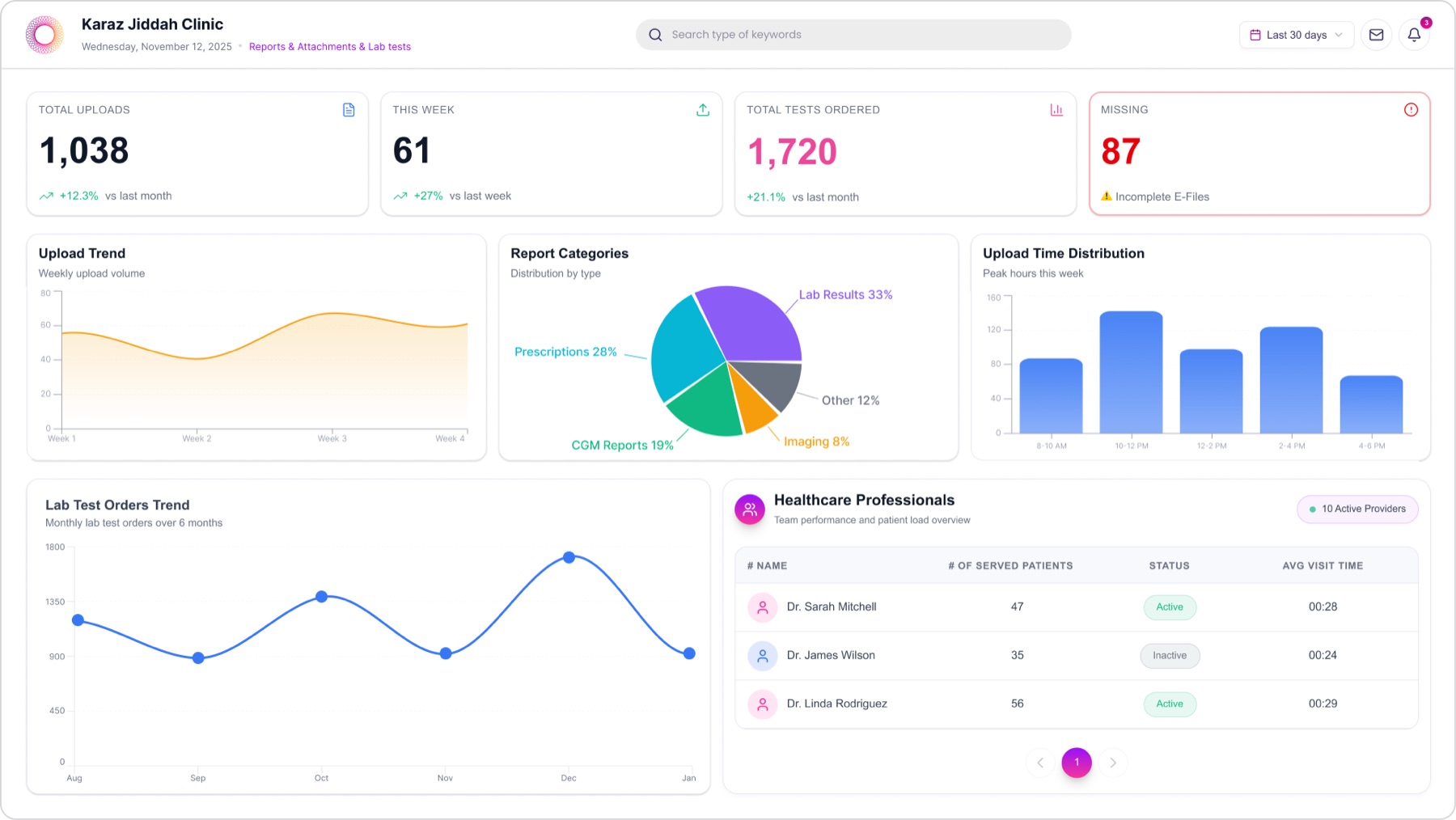
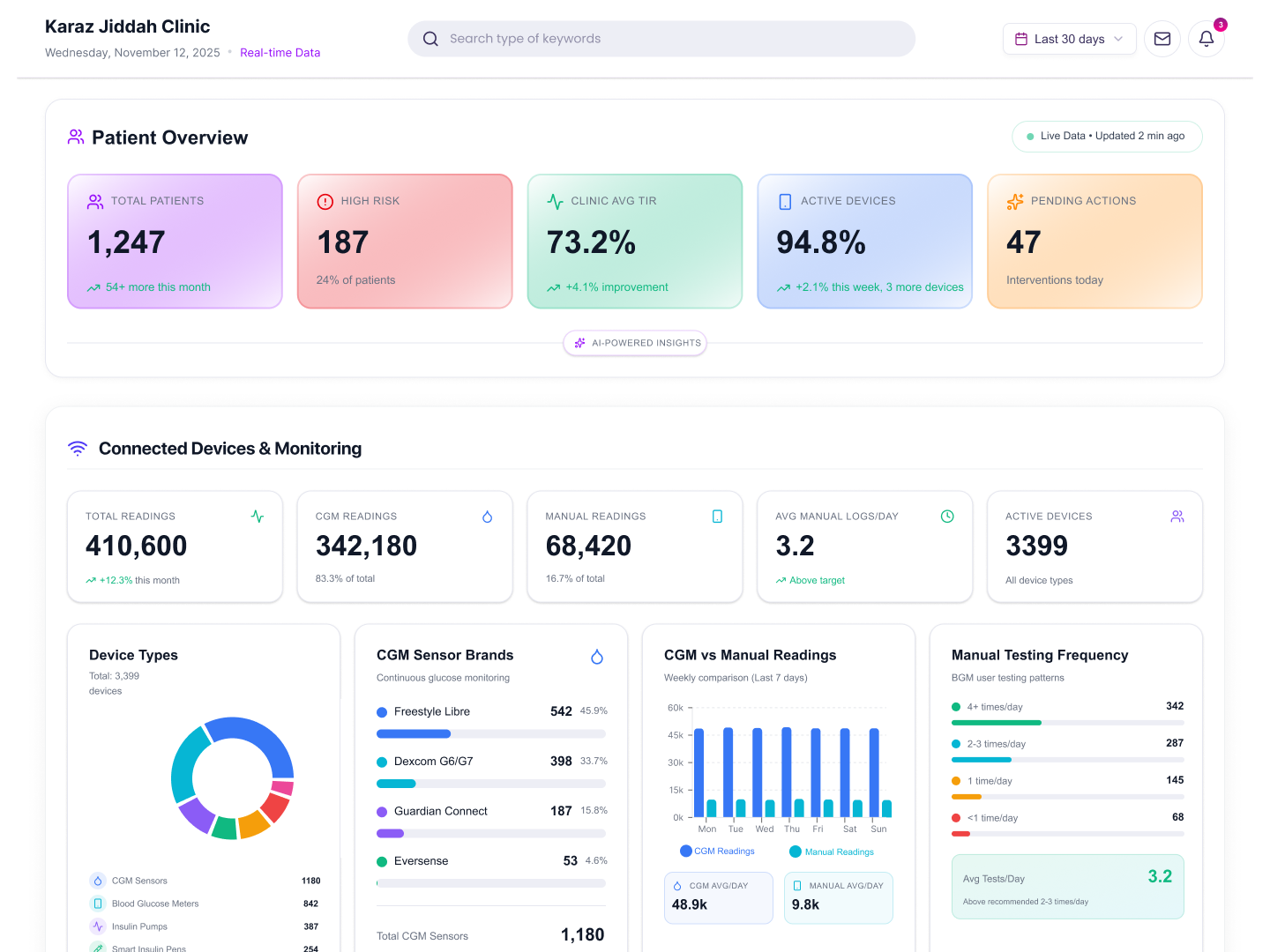
The Admin dashboard answers questions doctors do not need to think about. How many patients are active. Which devices are connected. Which clinical outcomes are improving. One long view, scrollable end to end, kept separate from clinical work so admins can see the clinic as a whole.
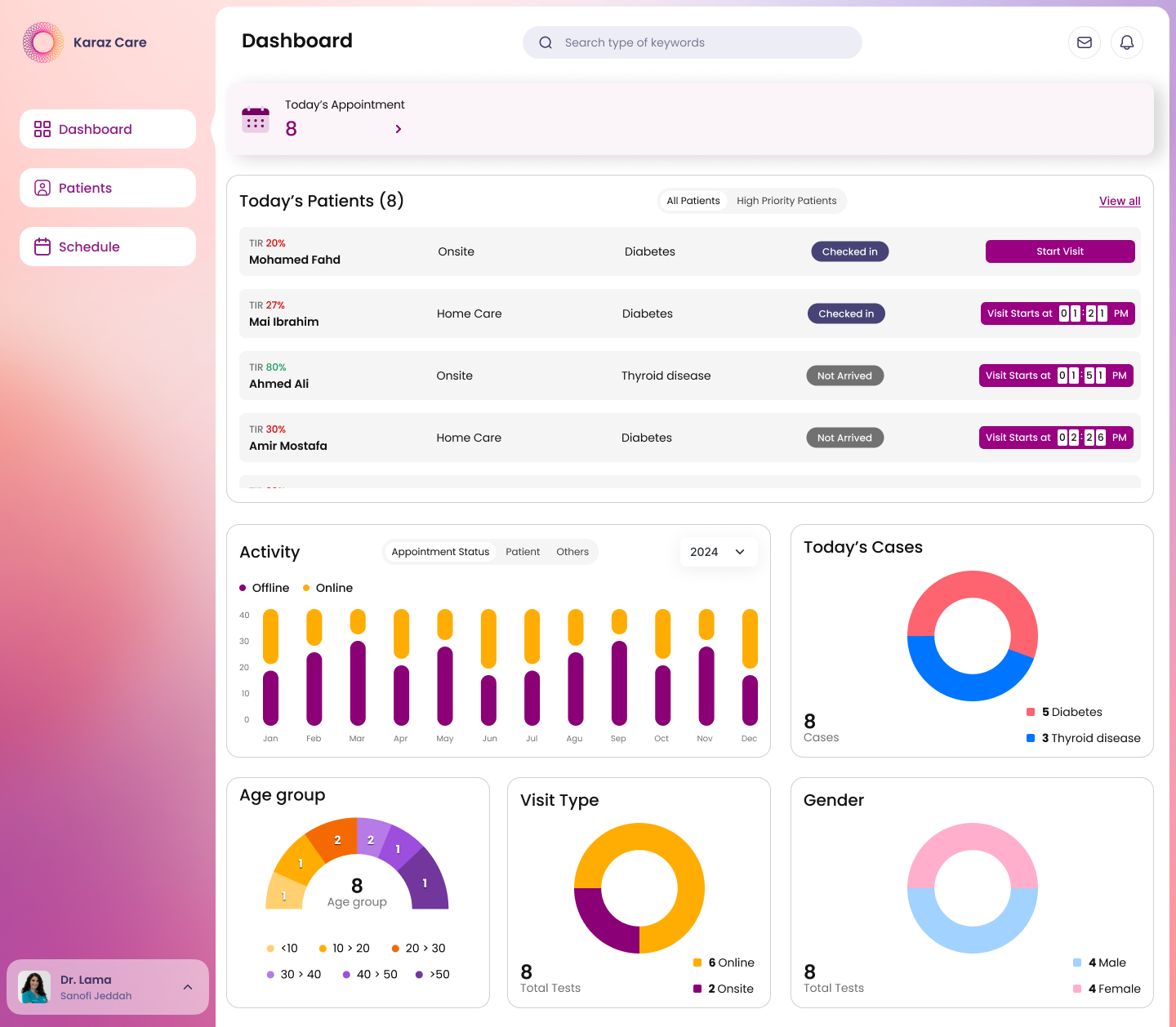
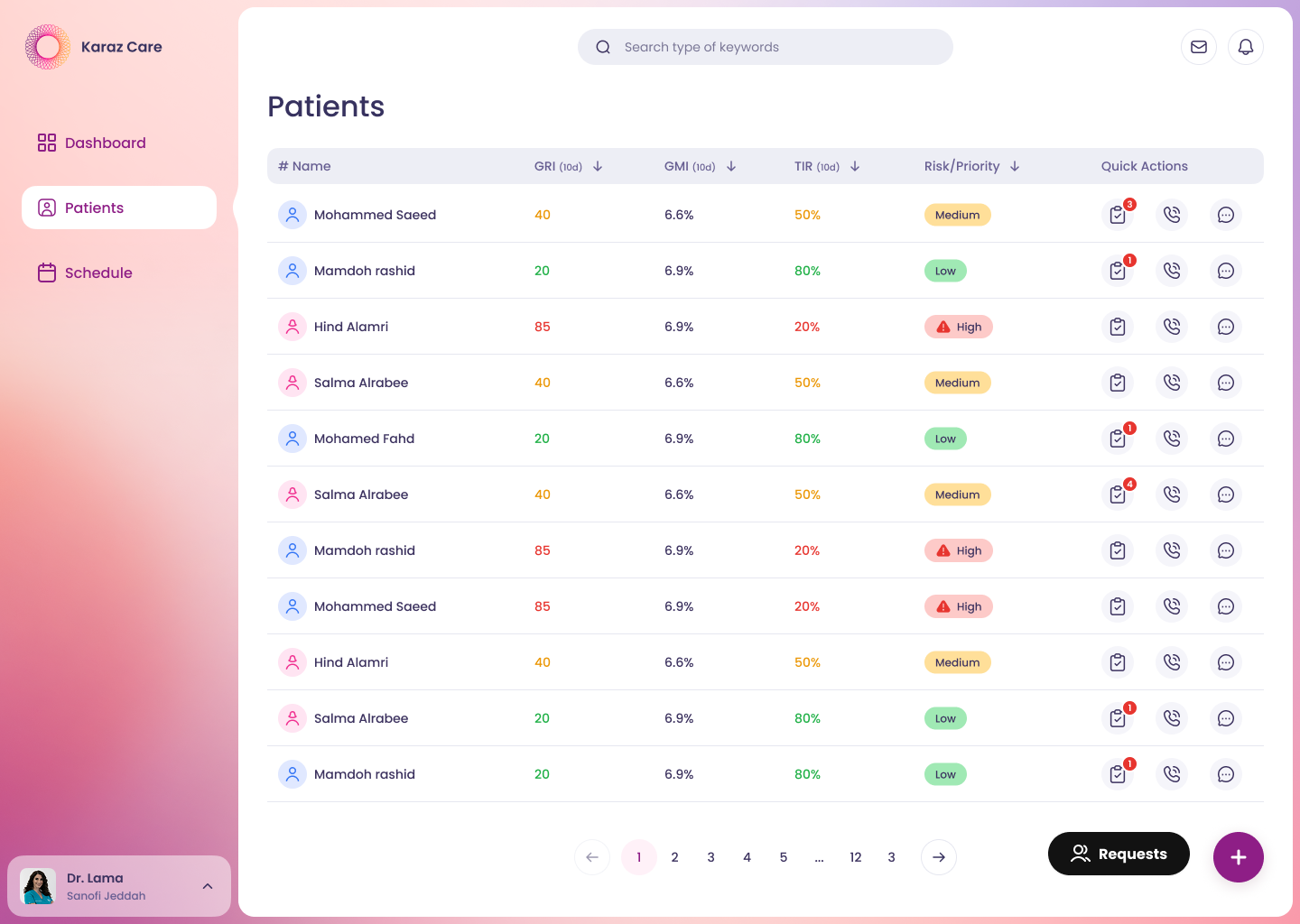
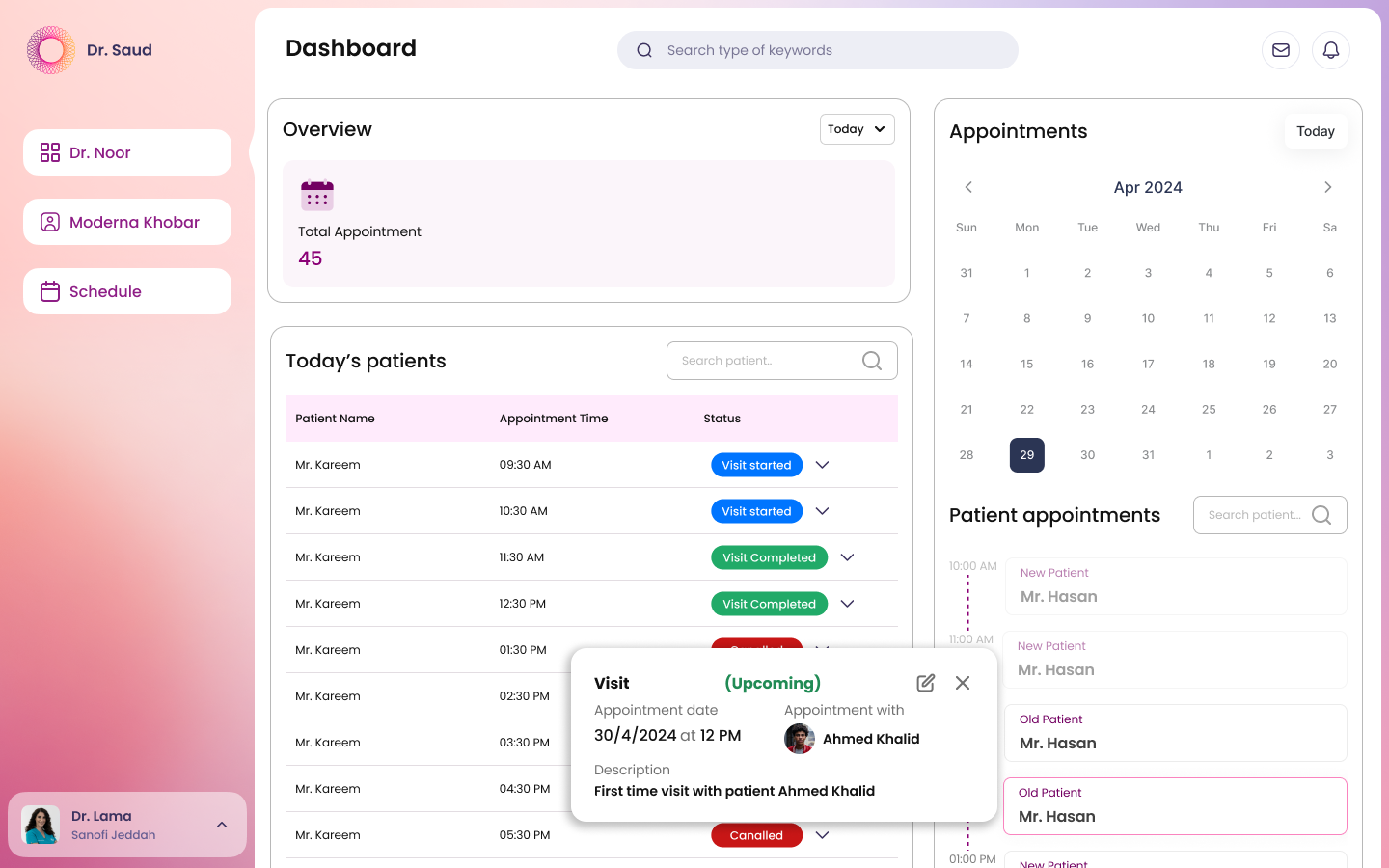
A doctor's day starts with the queue, not the database. The Doctor home opens with today's patient list — who is checked in, who is mid-visit, who is still waiting. From there, the doctor jumps to the full caseload, sorts by clinical risk, opens a single patient, and drills into Body Assessment, Medical History, and any attached report — all without leaving the page. Decisions, not data tours.
Receptionists run the visit pipeline, not the clinical record. The dashboard splits the day into three blocks: today's overview at the top-left, the patient queue with appointment times and visit status, and the appointments calendar on the right. Visit details open inline so the desk can confirm or reschedule without leaving the page. No clinical data clutters the view — what they need, nothing they don't.
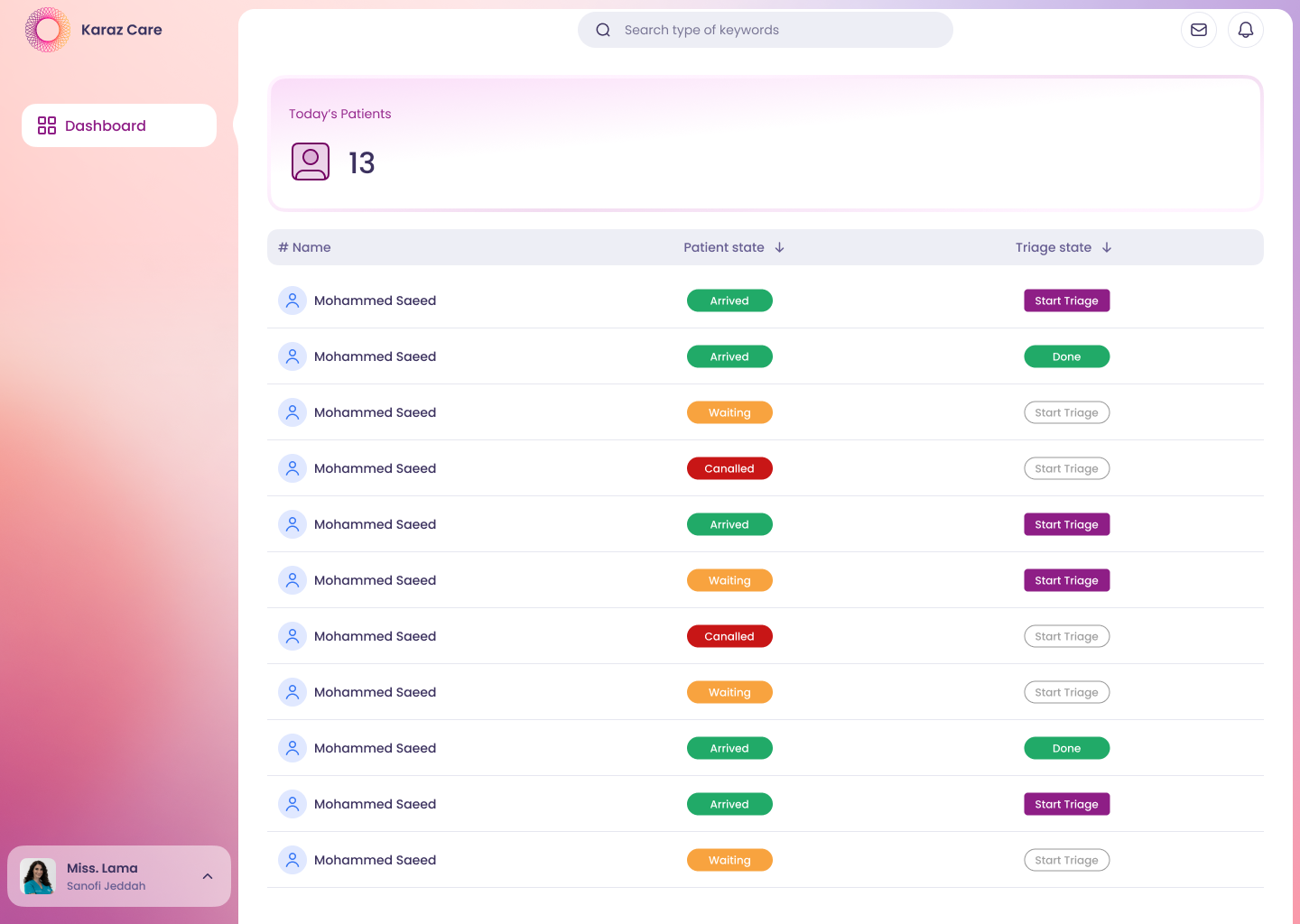
Nurses run the front of the visit. Today's patients in one list, with arrival state and triage state side by side. One screen, one job — start triage, mark done, move to the next.
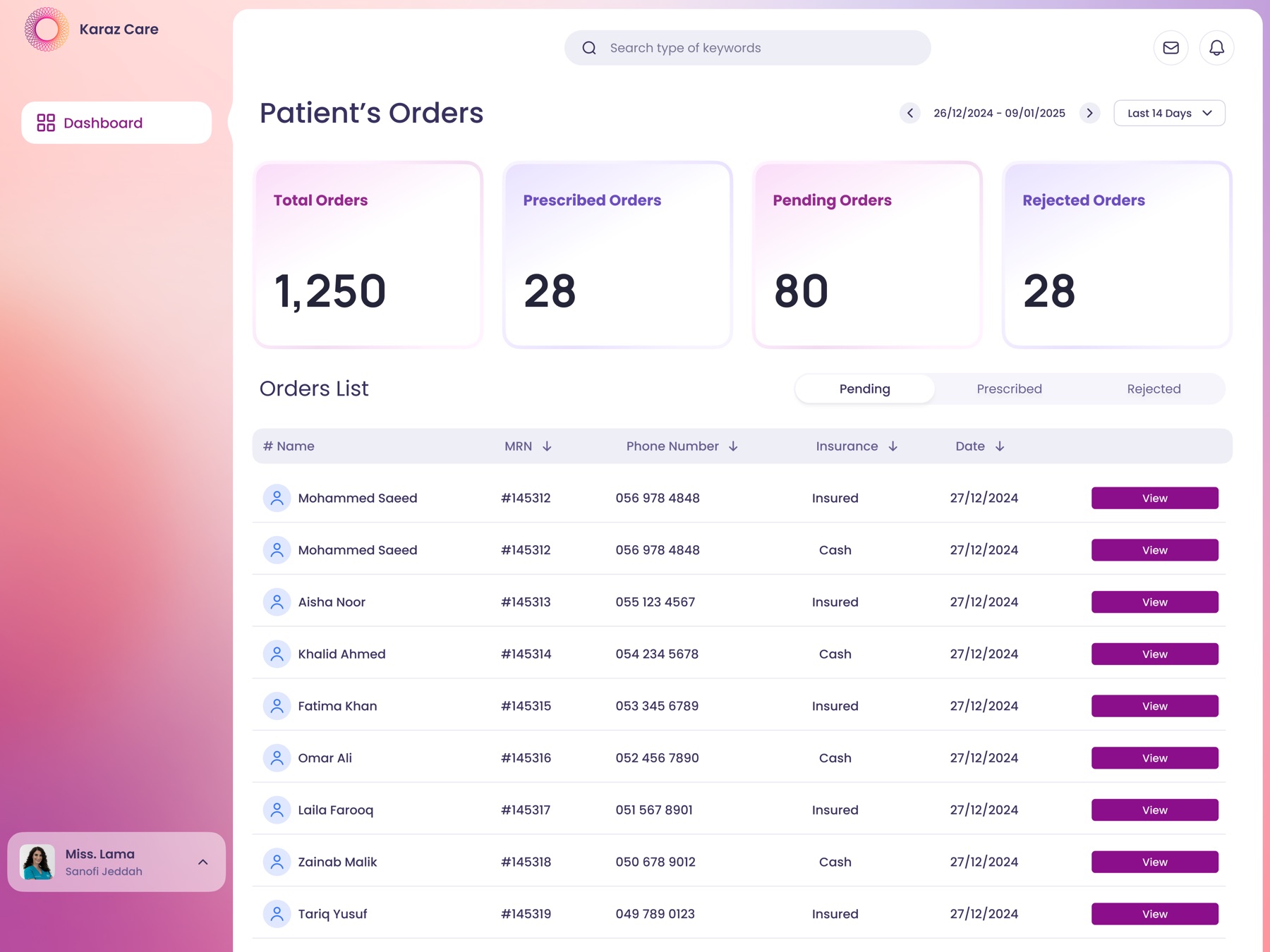
Pharmacy staff need a different kind of patient list. Their portal opens with the order queue — Total Orders, Prescribed, Pending, and Rejected as headline counts, then the orders list filterable by status in one tap. Each row carries the patient, MRN, contact, insurance type, and the View action that opens the full prescription. Separate from clinical risk so the team is not buried in noise that does not concern them.
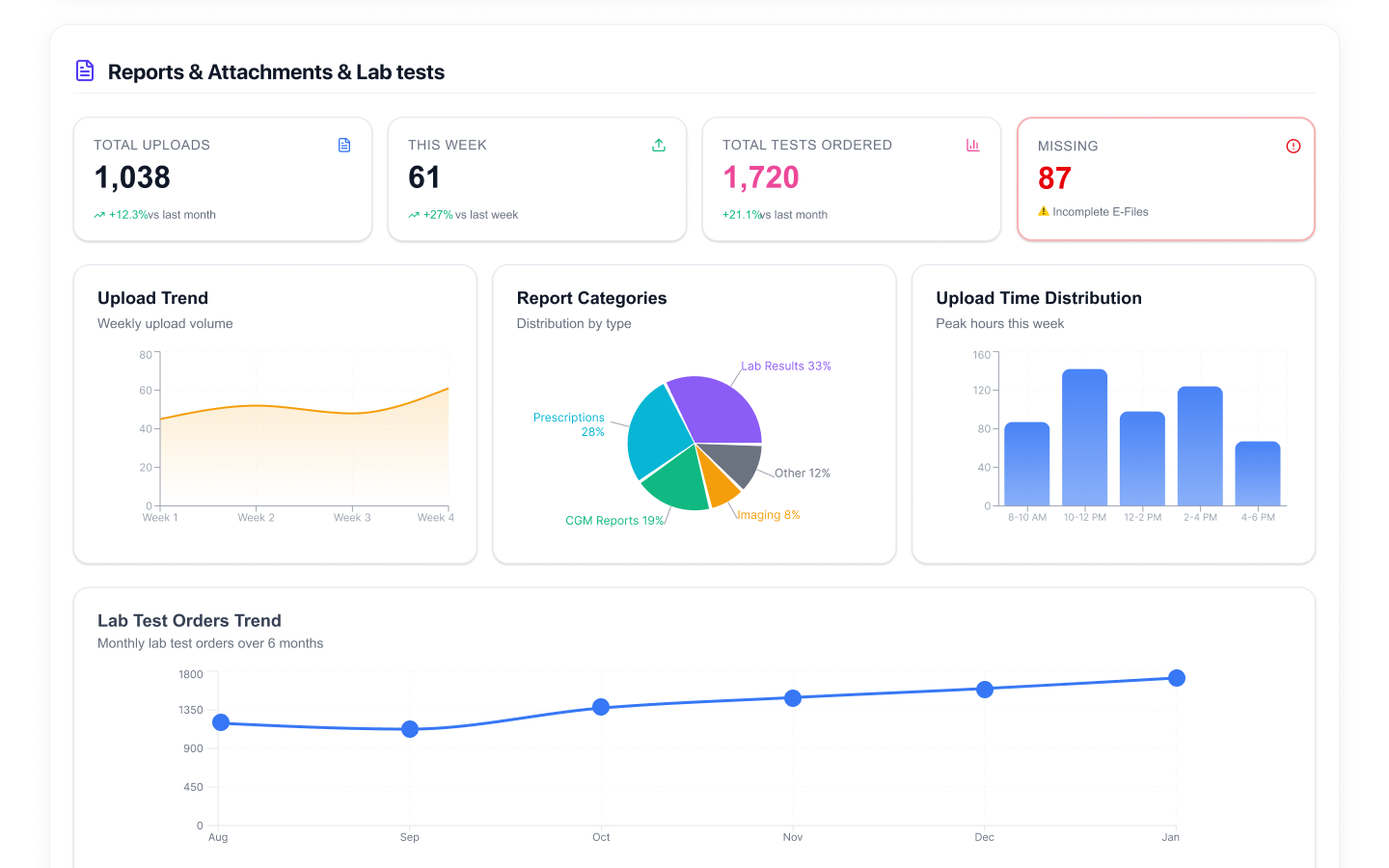
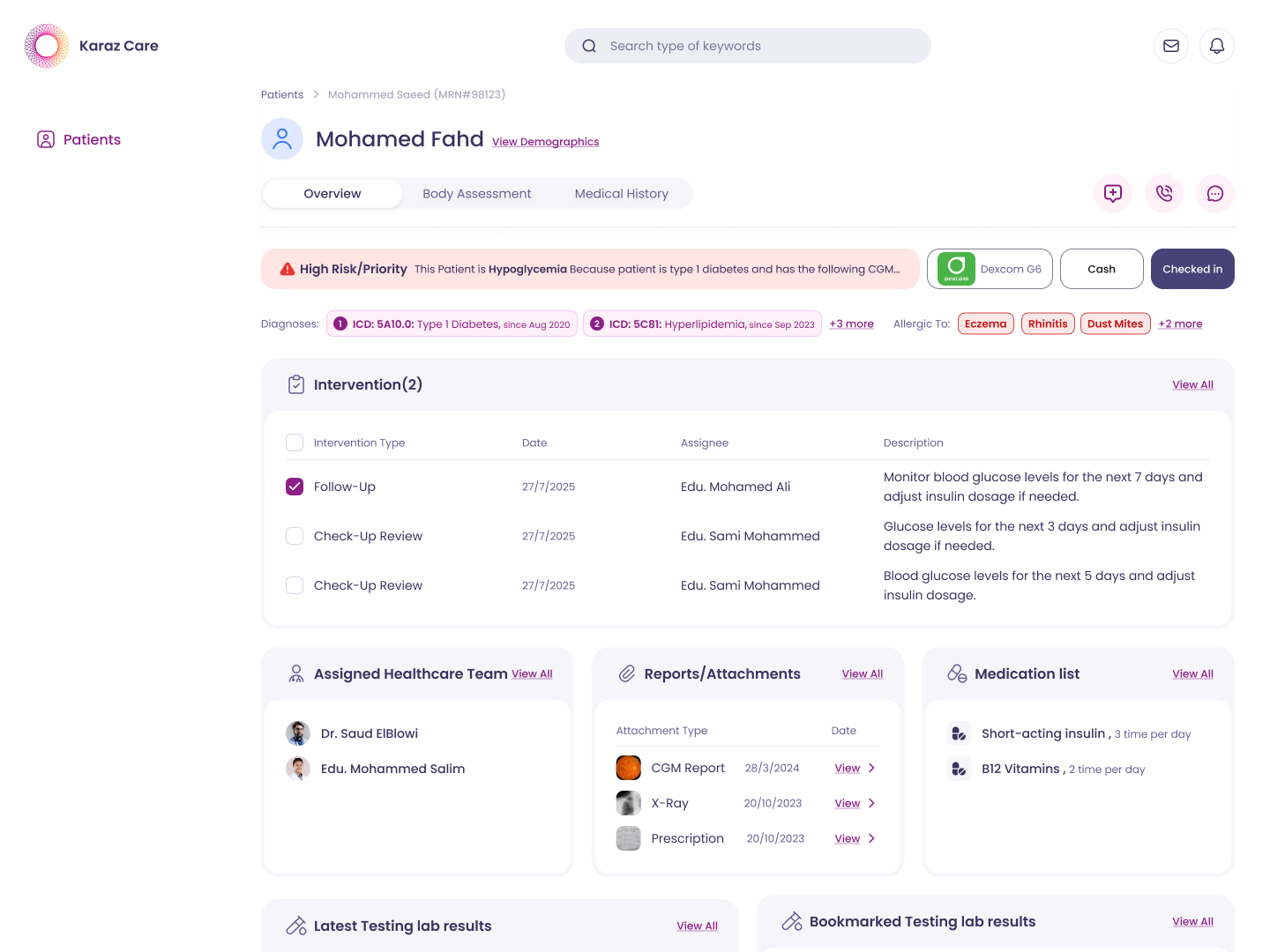
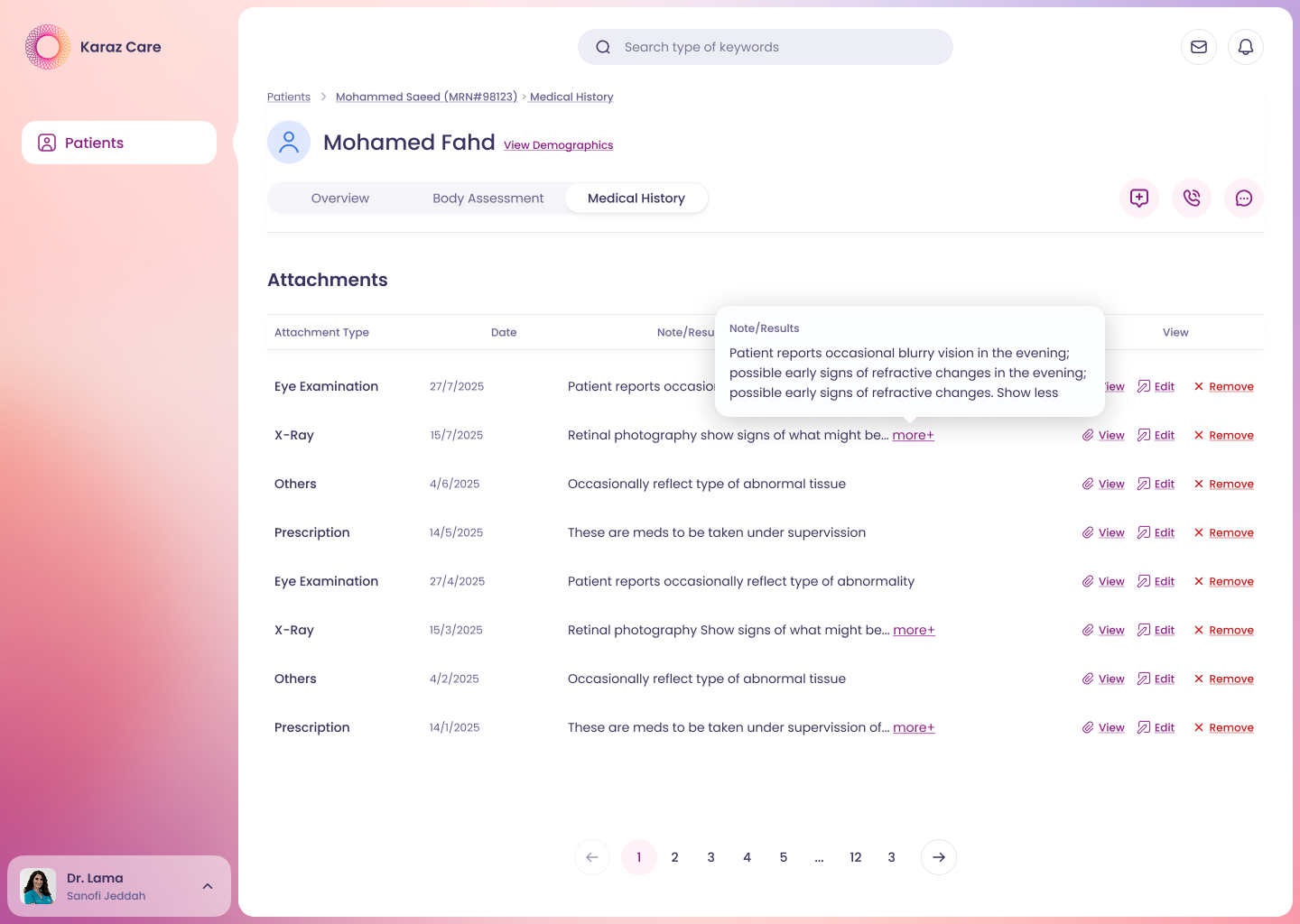
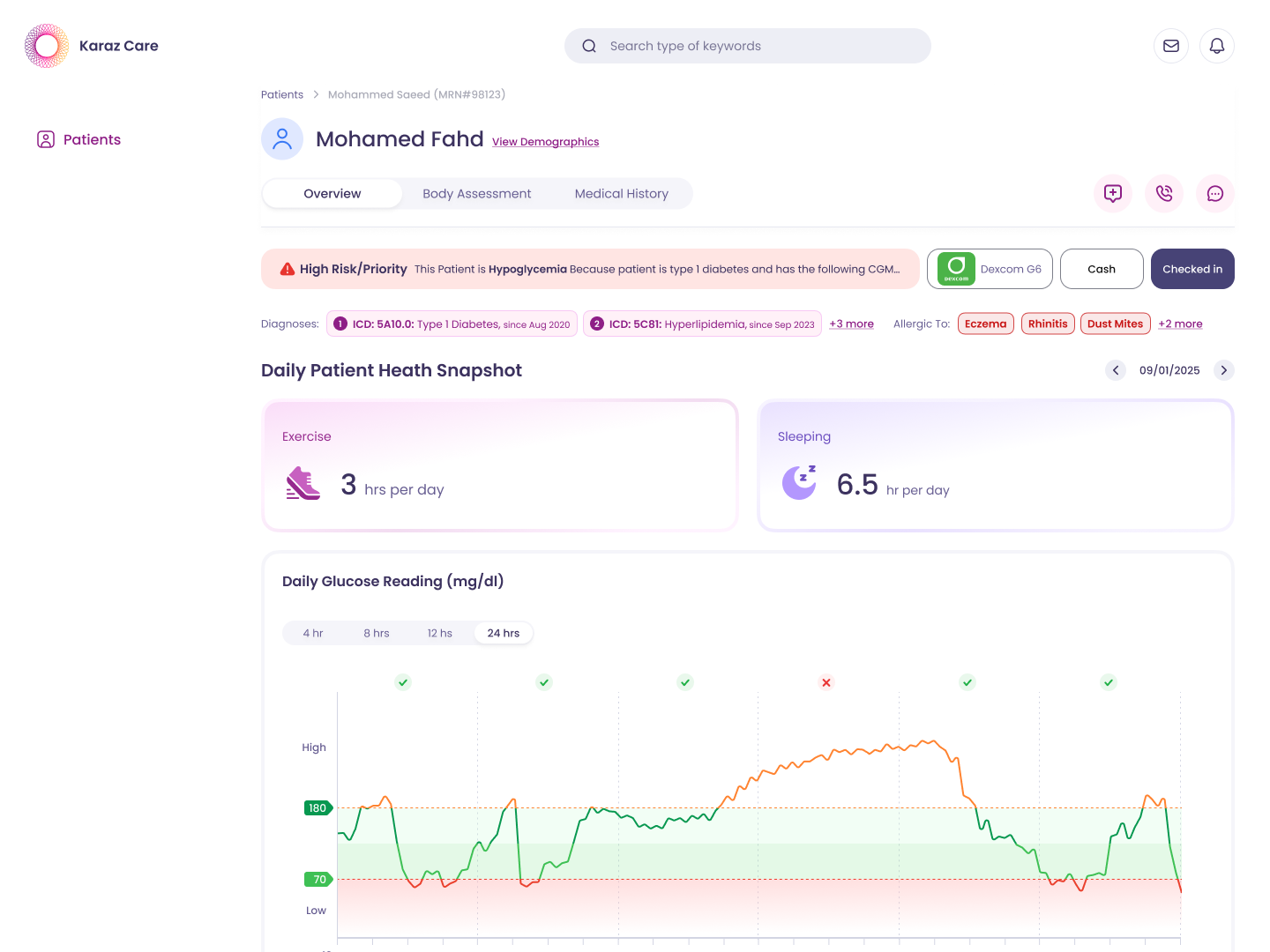
INSIDE THE PATIENT OVERVIEW
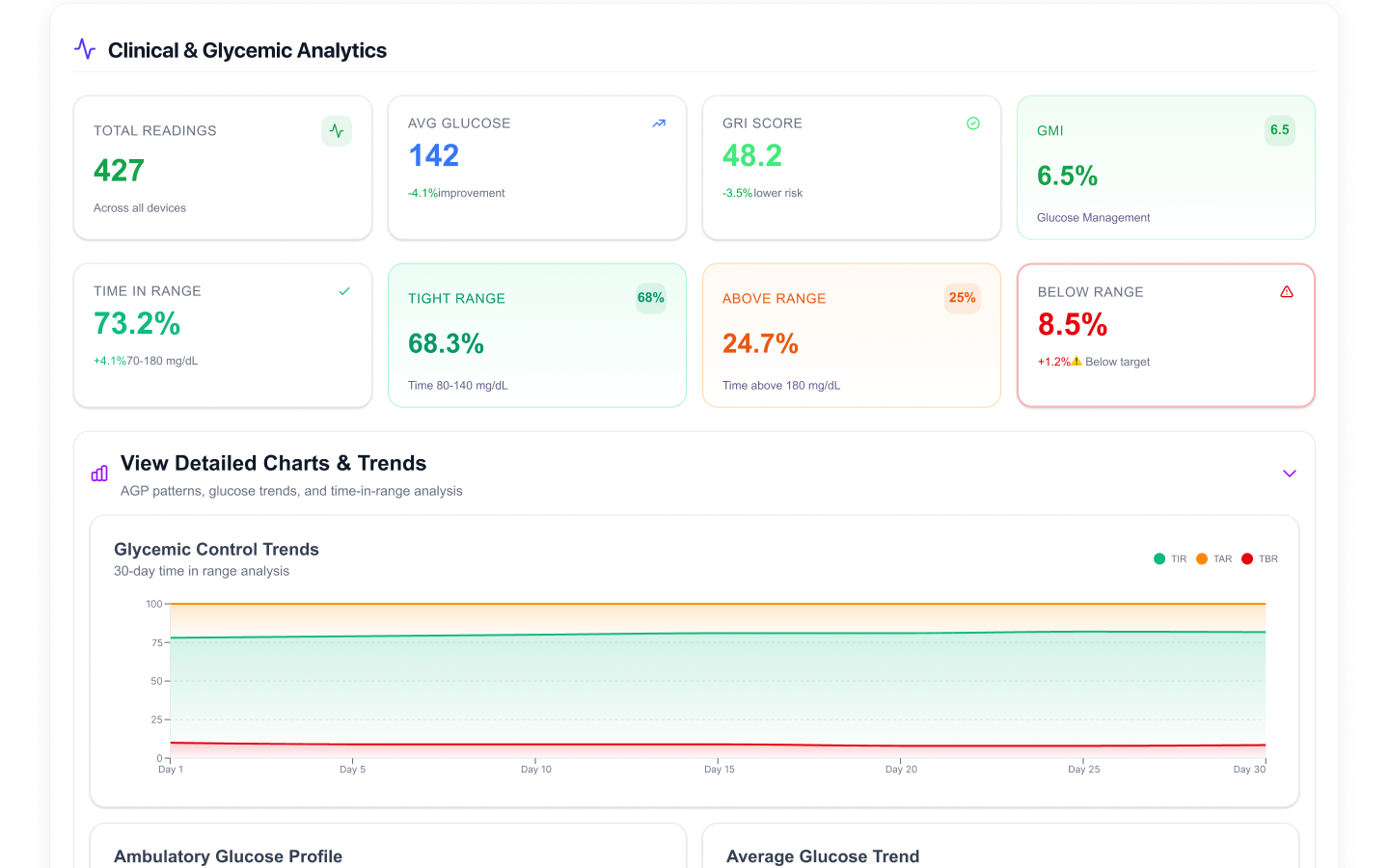
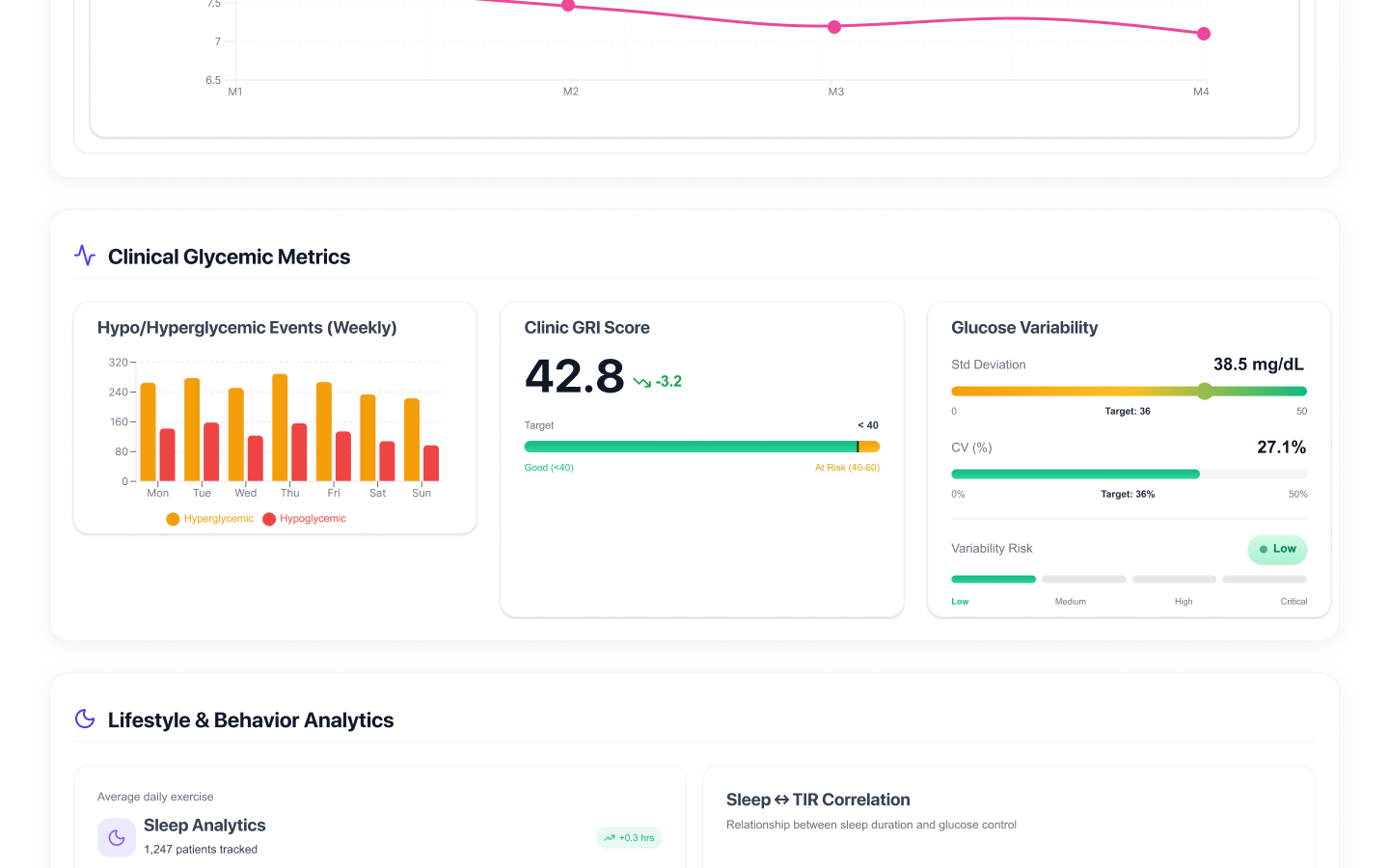
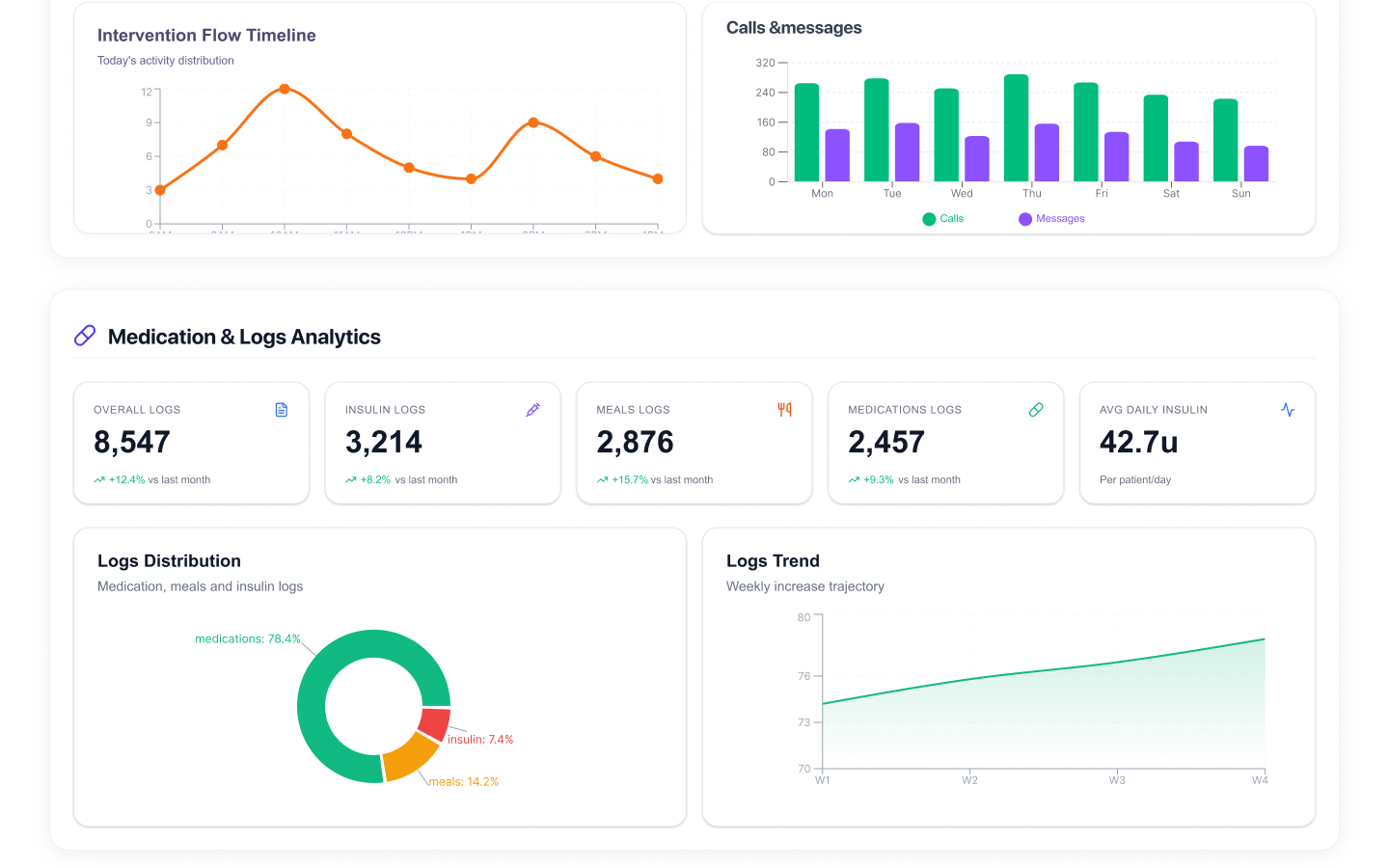
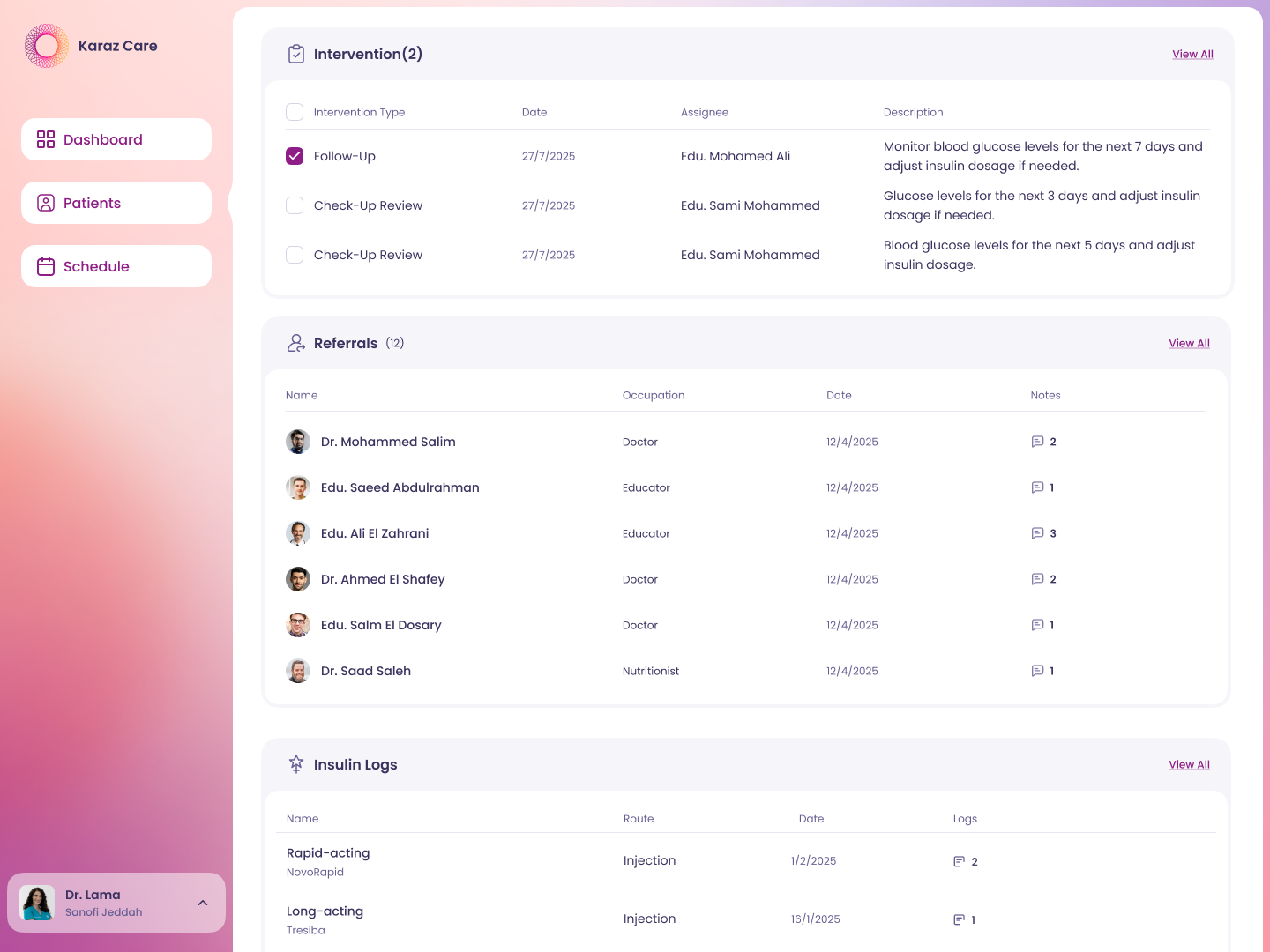
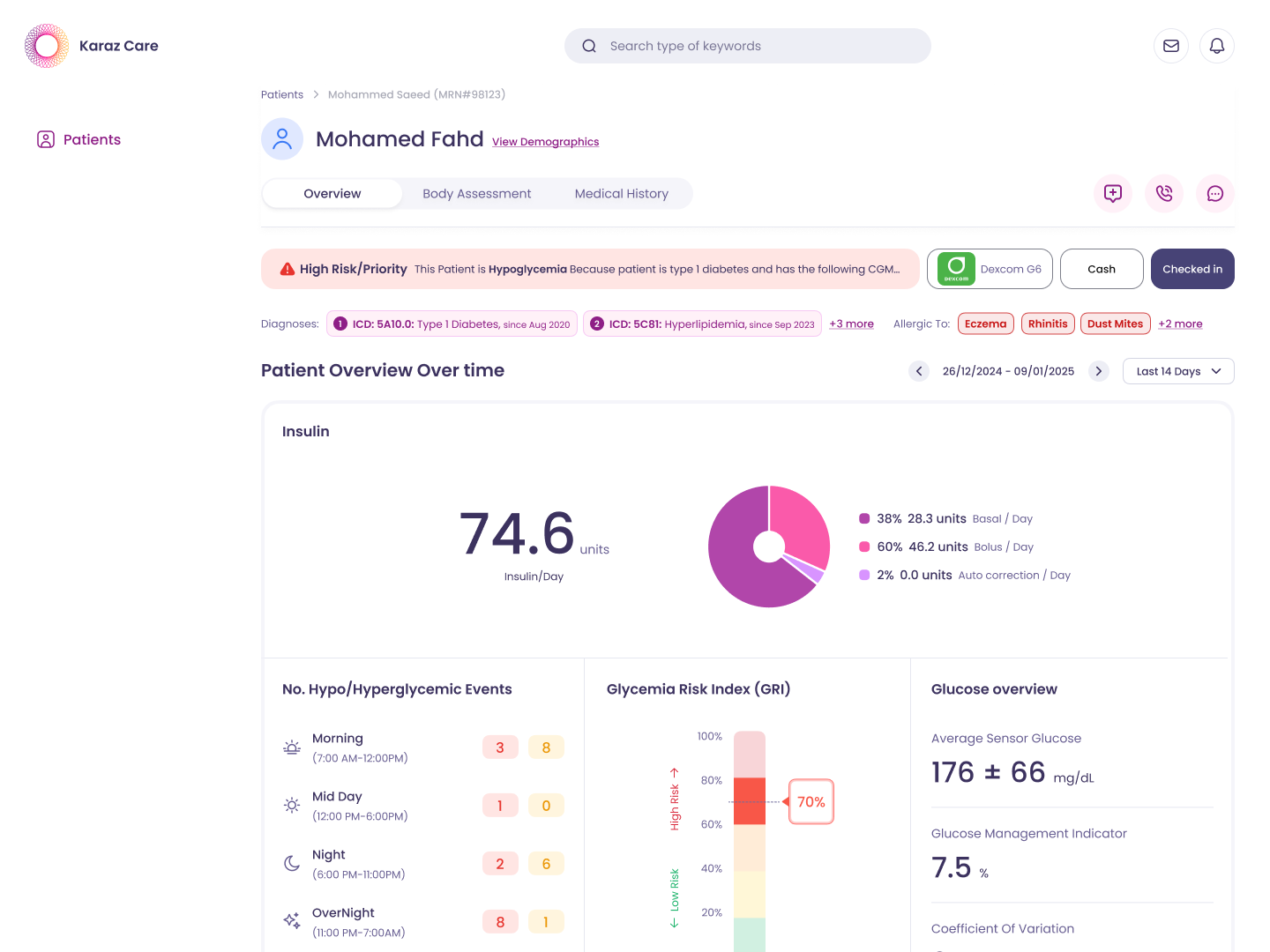
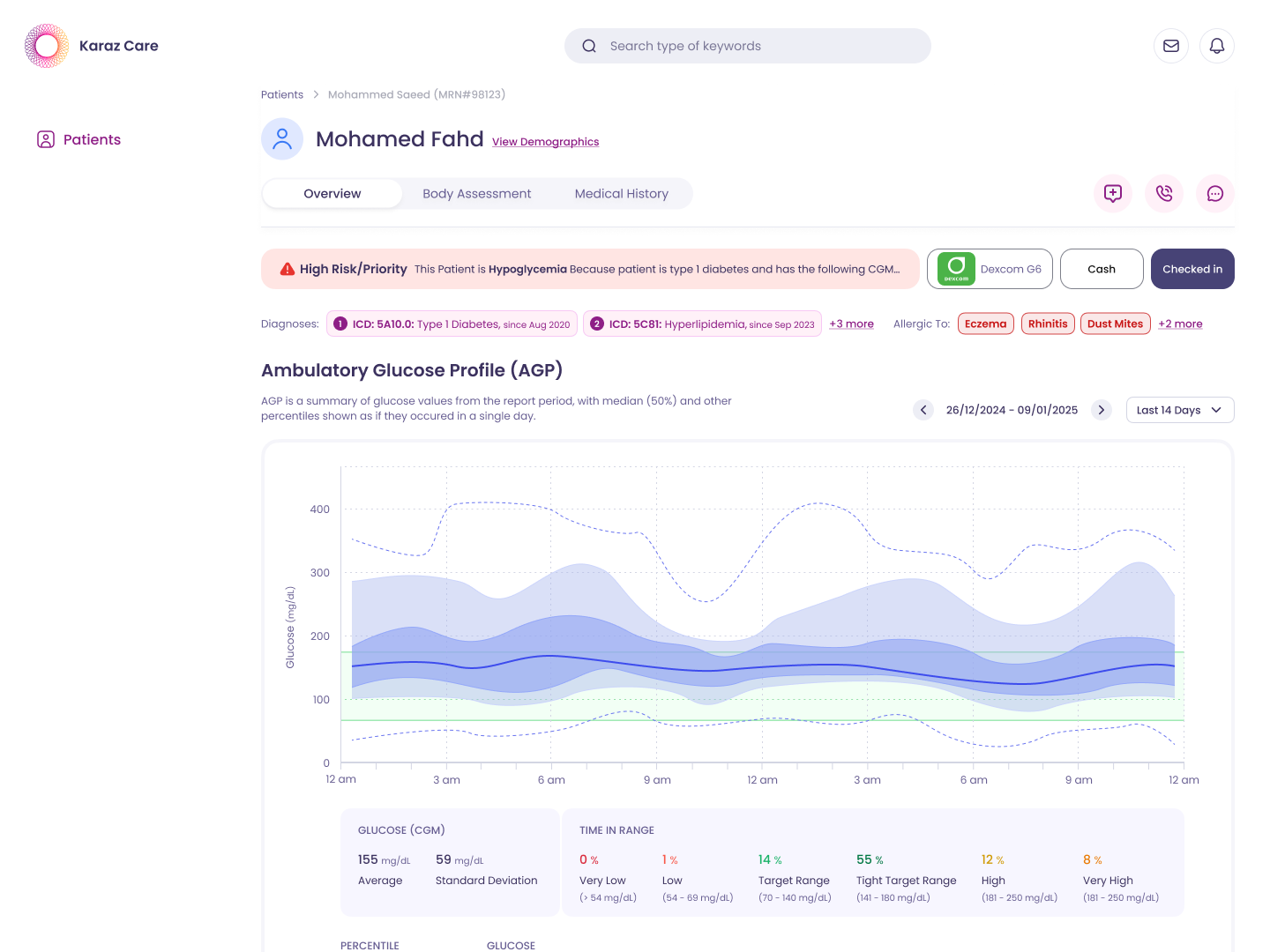
The patient record is one long view, scrollable end to end. Daily activity and glucose readings sit near the top. Insulin distribution and risk scoring come next. Then connected devices, ending with the ambulatory glucose profile. Each section answers a different clinical question without making the doctor leave the patient.
KEY DECISIONS
A receptionist managing waiting rooms and a clinician triaging risk see fundamentally different data. Forcing them into one dashboard hides what each role actually needs. I split the platform into five dashboards, each tuned to the decisions that role makes every day. Doctor sees risk. Receptionist sees waiting rooms. Admin sees clinic-wide stats. Pharmacy sees medication queues.
Built role-specific dashboards instead of one generic view. Each role solves different problems.
The Patient Overview needed eight quick actions — call, message, refer, add intervention, medicine, diagnosis, test, attachment. Putting eight buttons on the page would crowd the data, which is what clinicians actually came for. I tucked them into a single floating button that fans out on click. Actions are used a fraction as often as viewing the data, so they should occupy a fraction of the visual weight.
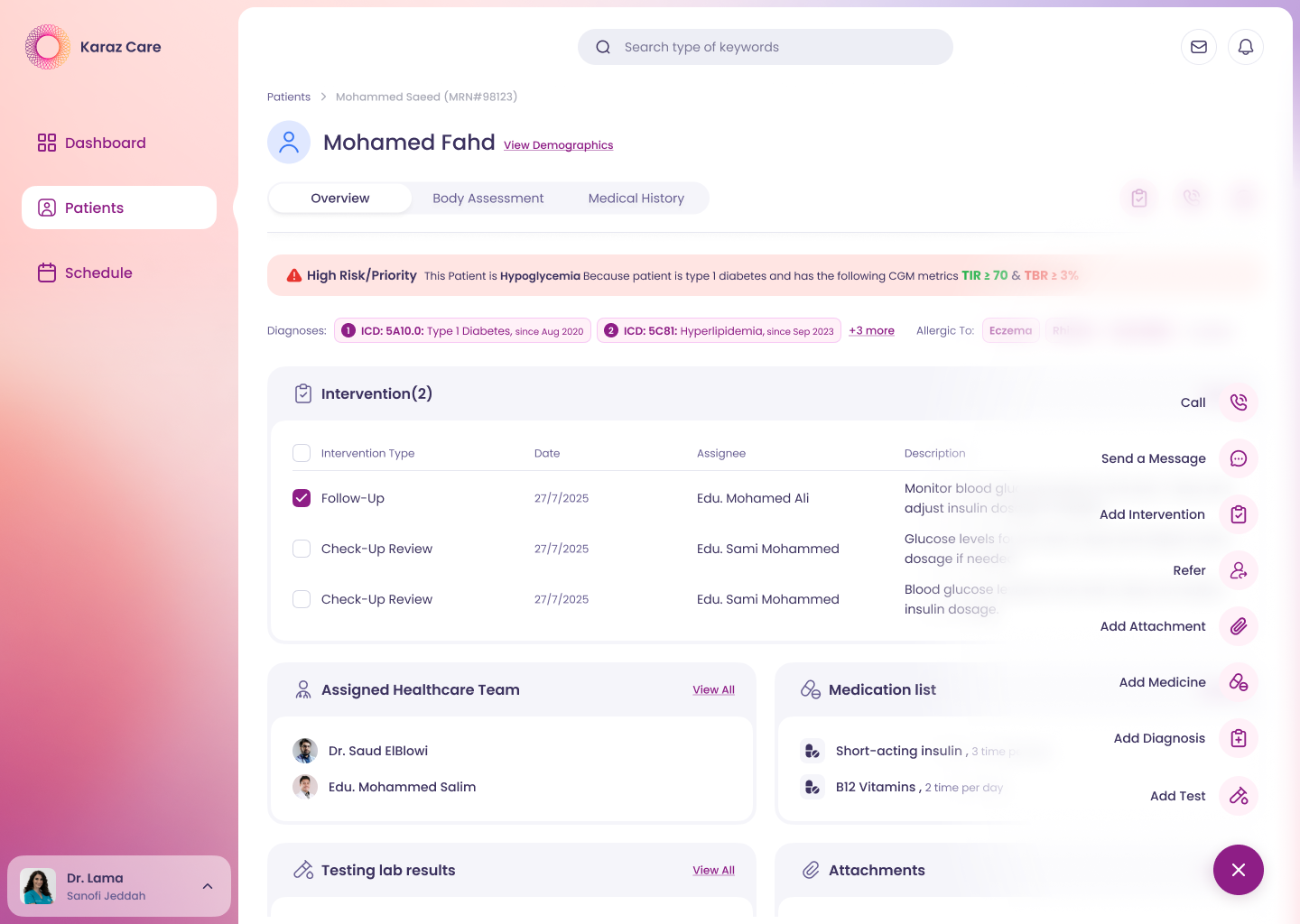
Hid 8 actions behind one button. Viewing data matters more than triggering actions.
A clinician seeing 100+ patients a day does not read a record top to bottom. They jump to one section, scan, and move on. One long scrolling page forces back-and-forth that wastes seconds on every visit. Three tabs — Overview, Body Assessment, Medical History — match how the data is actually used.
Three tabs over one long scroll. Clinicians don't read top to bottom. They jump and scan.
The High Risk banner could have just said "High Risk." Without context, it is just another dashboard the doctor has to interpret alone. Instead it reads in plain language: "This patient is Hypoglycemia because patient is Type 1 diabetic and has CGM metrics TIR ≥ 70 and TBR ≥ 3%." The why turns the screen from a data display into a decision tool.
Wrote the why into every risk flag. A flag without a reason is just noise.
The client and PM wanted every past lab result visible on the patient overview. I argued no. An overview that lists everything stops being an overview. We shipped recent results only, with a View All link to the full archive. The page kept its scanability, and clinicians could drill in when they actually needed history.
Pushed back on showing every past lab. An overview that lists everything stops being an overview.
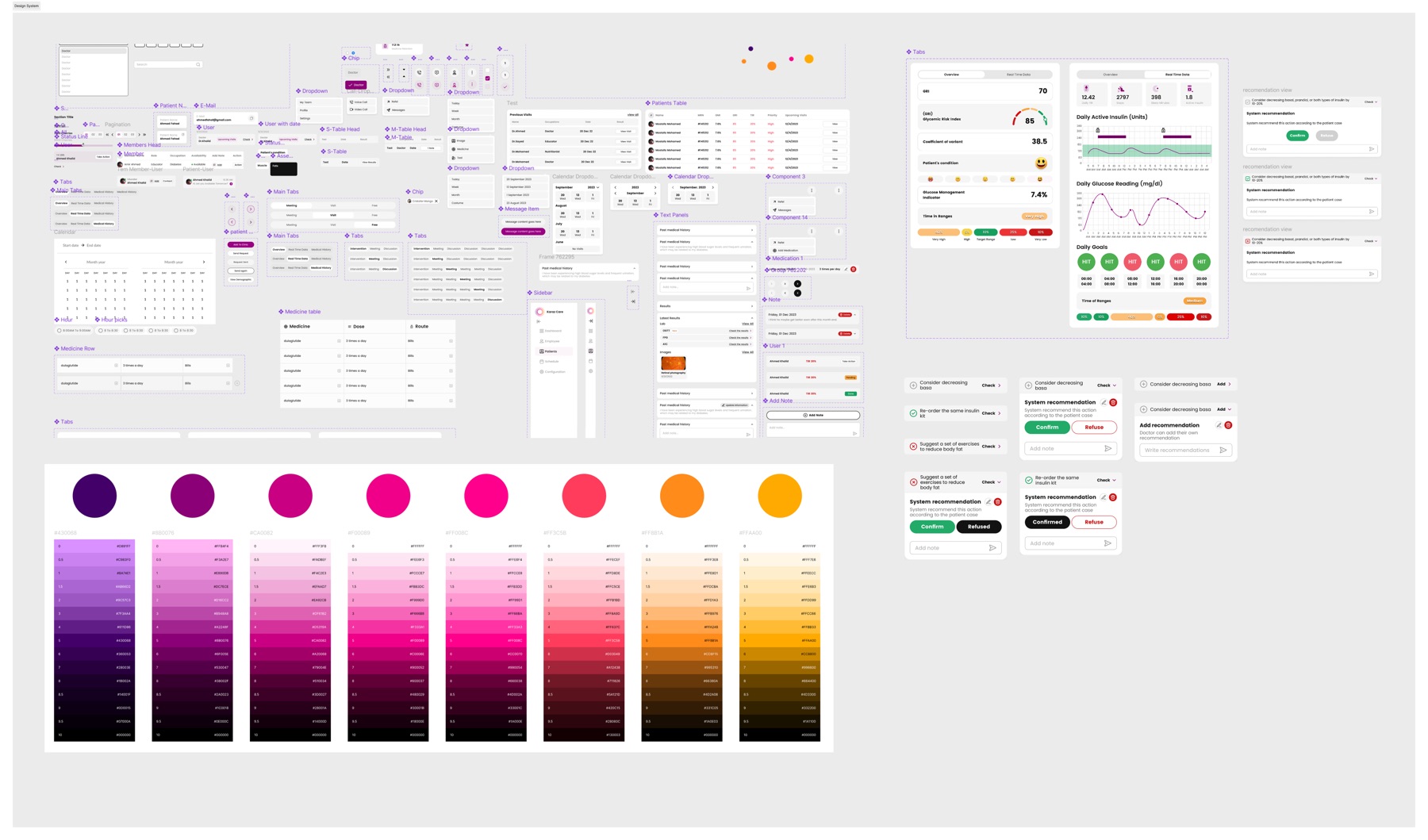
THE DESIGN SYSTEM
Five dashboards across one product means five places where inconsistency would have shown up immediately. A unified design system — colors, typography, components, icons — kept the platform coherent through every release. Engineers shipped faster because the spec was explicit, and new screens stayed visually accountable to the rest of the product.
HOW I WORKED
Model — Retainer. 4 months to v1, ongoing iteration after launch.
Communication — Daily standups on Slack. Direct line to the engineering lead and the client team.
Tools — Figma, ClickUp, Slack.
WHAT THIS MEANS FOR SIMILAR PROJECTS
Enterprise health tools fail when they treat all users as one. A receptionist, a pharmacist, and a doctor solve different problems. Designing for the role first, not the feature first, is what turns a database with a UI into software the team actually trusts.